Resistance to CTL-Mediated Killing
A key paradigm in HIV cure research is that the long-lived cells that harbor the HIV reservoir (and drive viral rebound if medication is stopped) are hidden from the immune system due to viral latency. Therapeutic strategies aimed at curing infection have thus focused on reversing latency, in order to expose these cells to the immune system, along with boosting immune cells (CTL and/or NK cells) to kill these exposed targets. This approach - termed “kick and kill” or “shock and kill” – is effective in model systems, but clinical trial results have thus far been disappointing.
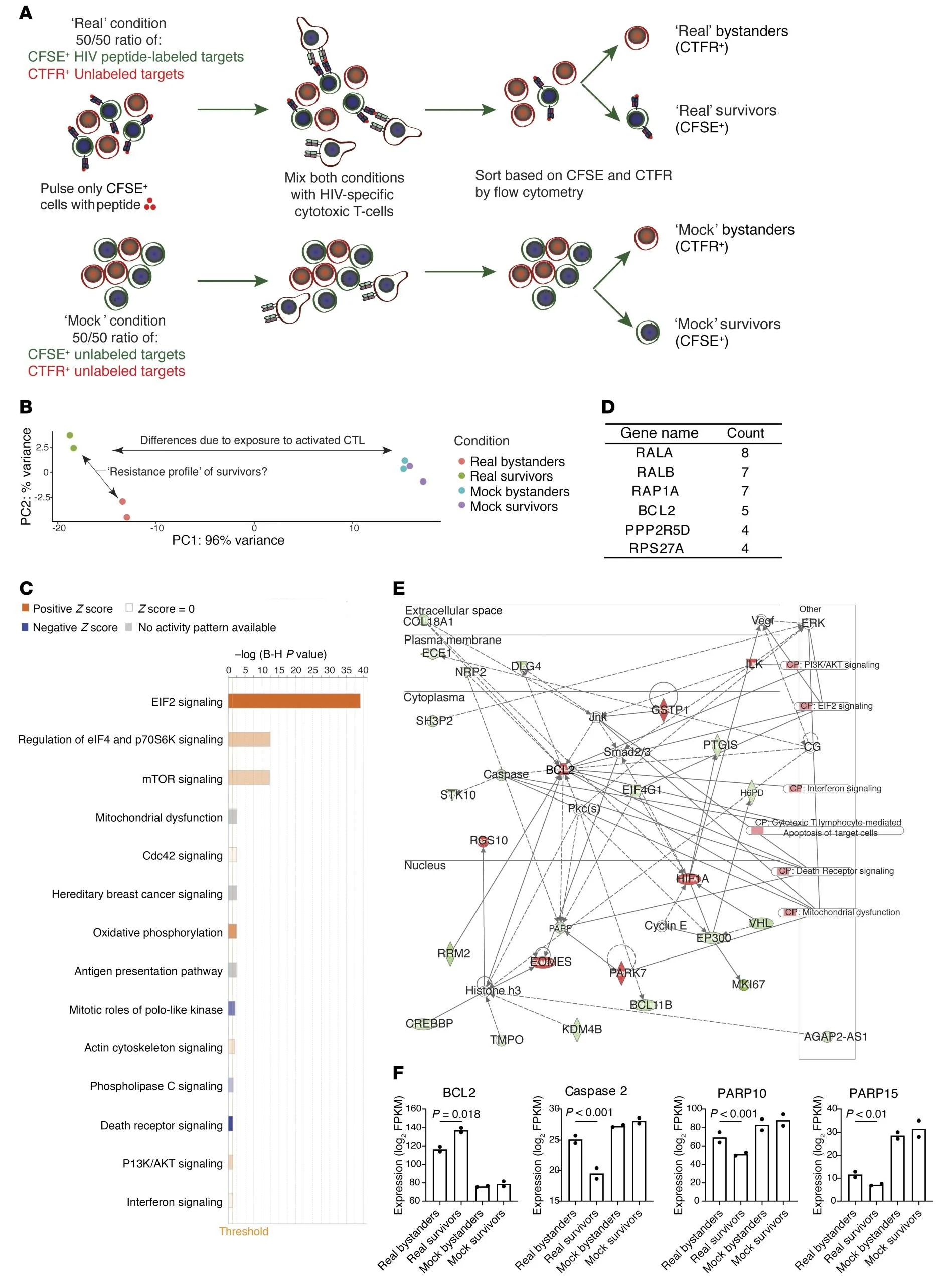
Results from our lab led us to posit that hiding from the immune system may not be the only way that reservoir-harboring cells can persist. Rather, we propose that some rare cells may have the intrinsic ability to resist being killed by CTL or NK cells - even when they are seen - and that these would selectively survive to form the persistent reservoir. Although largely unstudied in the context of HIV-infected CD4+ T-cells, mechanisms of CTL resistance are known in other settings (see inset Figure). Particularly in oncology, novel immunotherapy strategies have uncovered tumor cell resistance to CTL as a key factor limiting efficacy (1,2). Our studies thus far have identified over-expression of the pro-survival factor BCL-2 as one mechanism by which reservoir cells can resist killing, and that this can be counter-acted using BCL-2 antagonist drugs (3).
We hypothesize, however, that BCL-2 expression is likely to be only one of many factors that determine an infected cell’s intrinsic vulnerability to killing. Thus, a key focus of our research involves combining advanced CTL killing assays with cutting edge techniques, including transcriptomics, CRISPR screens, CITE-seq, CyTOF, and T-cell receptor/clonality profiling to both move us towards a comprehensive understanding of CTL resistance/susceptibility in HIV-infected CD4+ T-cells, and to identify potential therapeutic targets for testing against ex vivo reservoirs, in pre-clinical models, and potentially in clinical trials.
1 Restifo, N. P. et al. Loss of functional beta 2-microglobulin in metastatic melanomas from five patients receiving immunotherapy. J Natl Cancer Inst 88, 100-108 (1996).
2 Zaretsky, J. M. et al. Mutations Associated with Acquired Resistance to PD-1 Blockade in Melanoma. N Engl J Med 375, 819-829, doi:10.1056/NEJMoa1604958 (2016).
3 Ren, Y. et al. BCL-2 antagonism sensitizes cytotoxic T cell-resistant HIV reservoirs to elimination ex vivo. J Clin Invest 130, 2542-2559, doi:10.1172/JCI132374 (2020).